In comments over the weekend frequent commenter steve, IIRC an emergency medicine specialist, drew my attention to this post at The Incidental Economist. Take special notice of the graph.
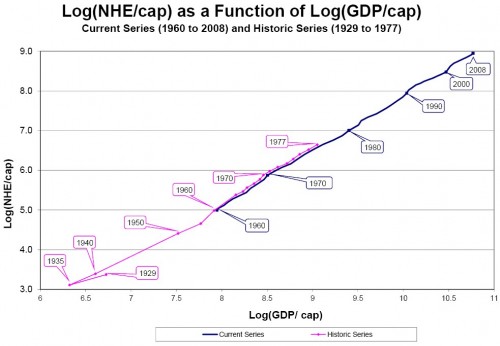
The graph is captioned “Log(NHE/cap) as a Function of Log(GDP/cap)”. The transliteration of that would be “the log of per capita national health expenditure as a function of the log of per capita gross domestic product” but that doesn’t really cast much light on it. It took me a while to formulate what I think is a reasonable translation of the chart into English: it’s an illustration of the rate at which healthcare expenditures per person are increasing relative to production of total goods and services per person over time (which is also rising). We know that’s the case because the slope of the curve is positive greater than 1.
The author of the post is right: it shows how tremendously persistent (and constant!) that rate has been over time and, consequently, how difficult changing that trend is likely to be.
I take some exception to this statement:
If, by action of politicians or the market, the health care spending curve is not bent, one might argue that this reflects our collective desire, our revealed preference. The history of health care spending in the US is consistent with the hypothesis that we view health care as a luxury good, one on which we spend more of our wealth as that wealth grows.
The argument for this interpretation would be a lot stronger if there were something that more closely resembles a market in healthcare and if those who paid for healthcare were the same individuals as those consuming healthcare. But there isn’t and they aren’t. Under the circumstances an equally reasonable interpretation of the chart that it illustrates the willingness of politicians to tax Peter to pay for Paul’s healthcare. Or the propensity of the healthcare industry to demand an ever-higher share of the national pie without producing commensurately more in actual results.
I can’t take a great deal of solace in the chart. It will be very difficult indeed to slow the growth in healthcare expenditures. The chart also sadly illustrates many of the problems we’re experiencing in our current economic doldrums: income inequality and slow growth in employment since the healthcare sector produces fewer jobs per marginal dollar spent than other sectors. Not that I’m blaming that solely on healthcare. The same is true in finance, education, and government, the other sectors that have seen substantial net job growth over the last decade or so.
But change it we will. Since roughly 60% of healthcare spending is derived, ultimately, from tax dollars and those tax dollars must come from somewhere, the healthcare sector requires not merely growing GDP but growing non-healthcare sector GDP.
What I think we should be most concerned about is a sector that has become too accustomed to a continually growing share of a shrinking, stable, or slowly growing pie. But that’s a subject for another post.
One last remark. I would genuinely like to see the historical series expanded at least to 1890. The creation of a healthcare oligopoly was a 20th century phenomenon, begun by the Pure Food and Drug Act of 1901 and reaching its fruition with the reforms advocated in the Flexner report of 1910. By 1935 when the historical series in the chart begins the medical profession had come to be dominated by post-Flexner physicians. I also think that the chart deals a deathblow to the rationale that healthcare expenses increase due to greater use of technology.






{kind=link}
Dave Schuler: We know that’s the case because the slope of the curve is positive.
Nitpick: We know it because the slope is greater than one, ~1.39. (It’s not clear in the graph because the x-axis is stretched compared to the y-axis.)
Dave Schuler: I can’t take a great deal of solace in the chart. It will be very difficult indeed to slow the growth in healthcare expenditures.
You might take solace in that many other developed countries have lower historical slopes, though they nearly all have some sort of universal healthcare system.
If you’d been reading my blog for a while or looked at my (many) archived posts on healthcare, you’d be aware that I’ve favored major healthcare reform in the U. S. for more than 30 years, either a single payer system or a full-on national health service. Unfortunately, either one of those require a political resolve to restrain healthcare costs, something I think is lacking.
Do you see something in the national dialogue which suggests to you that a political consensus is about to form around a system that will restrain healthcare costs? I don’t.
I think it also bears mentioning that we’re very different from other OECD countries, much more diverse in race, ethnicity, religion, and so on (although, oddly, not in politics). The more homogeneous the population the more likely the country is to pursue policies like a single-payer healthcare system or national health sstem.
Dave Schuler: If you’d been reading my blog for a while or looked at my (many) archived posts on healthcare, you’d be aware that I’ve favored major healthcare reform in the U. S. for more than 30 years, either a single payer system or a full-on national health service. .
Sure. The graph shows why the current system is unsustainable over the long run. Solace is found in understanding that the slope is not inevitable—the first step towards finding a solution.
Dave Schuler: Do you see something in the national dialogue which suggests to you that a political consensus is about to form around a system that will restrain healthcare costs? I don’t.
Not yet. The solution the U.S. will eventually adopt will probably combine aspects of private and public pay, which will help address the heterogenous nature of American society.
That’s essentially the system we’ve got which, as you point out, is unsustainable.
And they don’t solve the problem. It mitigates the problem, but places like the UK, Canada, France, etc. will tell you that health care costs are rising at an unsustainable pace.
As Dave notes that is what we have now. If anything that is part of our problem.
There are several things of interest in that graph. Yes, the slope is positive, but it is also nearly a straight line. I was surprised that we did not see big jumps when Medicare started or when Medicaid started. Health care spending just keeps going up steadily, related mostly to GDP, no matter what.
I would not rule out technology changes. Antibiotics hit the scene in the early 40s. Prior to that, medicine did not have that much to offer. Before Flexner, docs were mostly shamen.
“The argument for this interpretation would be a lot stronger if there were something that more closely resembles a market in healthcare and if those who paid for healthcare were the same individuals as those consuming healthcare.”
It takes on that straight line before govt gets involved in paying for health care. Before business really started paying for workers health care.
“I can’t take a great deal of solace in the chart. It will be very difficult indeed to slow the growth in healthcare expenditures. ”
It was not intended to provide solace, it should worry everyone. With differing levels of govt involvement, with different political parties in charge, this relationship stays constant.
Steve
Steve Verdon: And they don’t solve the problem. It mitigates the problem, but places like the UK, Canada, France, etc. will tell you that health care costs are rising at an unsustainable pace.
Yes, but they start at a lower point and are rising more slowly.
Steve Verdon: As Dave notes that is what we have now. If anything that is part of our problem.
The traditional U.S. system doesn’t have a very good mechanism for controlling costs. It basically enables the worst features of the market system while trying to guarantee care for a large sector of the population.
Nearly all advanced economies have some sort of universal care, but they may be public insurance-public providers (U.K.), public insurance-private providers (France), or private insurance-private providers (Switzerland).
steve: It was not intended to provide solace, it should worry everyone. With differing levels of govt involvement, with different political parties in charge, this relationship stays constant.
Well, it should be a call to action. The first thing the U.S. should do is look at other systems that are more effective. They all require universal coverage, as the public ends up paying one way or another.
Okay Zachriel I don’t think you quite understand the point. Switching systems wont make health care spending sustainable. In fact, it isn’t even clear to me it will help here in the U.S. It might, but it is a debatable position. Right now there is no solution.
Bahahahahaha…whew…wait, not done…hahahahahahahaha…man, that was funny.
What might be effective in Country X may not work too well here. Many countries that have systems that are working are smaller, for instance. There maybe a cultural aspect at work as well. We’ve gone down this road here at Dave’s site and over at Outside the Beltway.
The bottom line is that the prognosis is very grim. As frequently as I disagree with steve, I agree with his last paragraph…nothing will change. This thing will run off the rails first wreaking havoc on not just our economy, but probably the world economy. Add on Social Security, the possibilities for sovereign debt crises, and things look very fun indeed for the next decade.
steve,
Dude, it is in logs. What is key is that the slope of the “straight line” is greater than 1. That means that as GDP goes up, as a society, we allocate an increasing share of GDP towards health care.
You would only expect to see a jump if Medicare was a one time increase in spending. It probably wasn’t just that. It was most likely a small increase, but also a change in growth rate of spending as well, hence you’d expect to see a change in slope, which is precisely what I see in that graph around 1960 relative to the historical series.
Yes, so what? If we adopt one of their systems will our healthcare costs be lowered to the OECD average and then rise at the more modest, but still unsustainable, OECD rates? No – the best we could hope for is reduced marginally reduced cost growth.
Steve V is right that there are other factors involved. One can’t just adopt, for instance, Finland’s program (population 5 million) and expect it to work in a diverse country of 300 million. The US isn’t a nation-state like most European countries – we are a political union which is a much different animal.
“see a change in slope, which is precisely what I see in that graph around 1960 relative to the historical series.”
Medicare was passed in 1965 with spending really taking hold in 1970. If there is any change in slope, it is minimal. If government spending is driving health care costs, why dont we see a change in slope you can find w/o a protractor?
Steve
My tentative answer is that the constant acceleration is the result of policy without which healthcare as a proportion of the economy would have declined.
I gather that Steve V.’s answer is that the data prior to 1965 aren’t very good.
Steve Verdon: Right now there is no solution.
As other countries have lower costs and lower growth in costs, that would seem to indicate there is something different about the American situation. What would that be?
Steve Verdon: Many countries that have systems that are working are smaller, for instance.
Well, that’s the point. Western Europe has universal coverage, yet pays less for comparable results.
Steve Verdon: No – the best we could hope for is reduced marginally reduced cost growth.
Lower growth is essential, of course.
Steve Verdon: The US isn’t a nation-state like most European countries – we are a political union which is a much different animal.
Western Europe is an even looser political and broader cultural affiliation, yet has universal coverage. The U.S. has many advantages, including economic and a single, national culture. The problem is political, as well as economic. The U.S. system requires supermajorities for any major change, and has much looser political cohesion.
Steve Verdon: My tentative answer is that the constant acceleration is the result of policy without which healthcare as a proportion of the economy would have declined.
Part of it is technological, and part of it is a component of a wealthier society that has more to spend on marginal improvements in health care. But the U.S. is simply overpaying for what they receive in terms of benefits.
Sorry. Messed up the attribution above. Here it is again.
Steve Verdon: Right now there is no solution.
As other countries have lower costs and lower growth in costs, that would seem to indicate there is something different about the American situation. What would that be?
Steve Verdon: Many countries that have systems that are working are smaller, for instance.
Well, that’s the point. Western Europe has universal coverage, yet pays less for comparable results.
Andy: No – the best we could hope for is reduced marginally reduced cost growth.
Lower growth is essential, of course.
Andy: The US isn’t a nation-state like most European countries – we are a political union which is a much different animal.
Western Europe is an even looser political and broader cultural affiliation, yet has universal coverage. The U.S. has many advantages, including economic and a single, national culture. The problem is political, as well as economic. The U.S. system requires supermajorities for any major change, and has much looser political cohesion.
Dave Schuler: My tentative answer is that the constant acceleration is the result of policy without which healthcare as a proportion of the economy would have declined.
Part of it is technological, and part of it is a component of a wealthier society that has more to spend on marginal improvements in health care. But the U.S. is simply overpaying for what they receive in terms of benefits.
Zachriel,
Probably a number of things. Here are some, in no particular order….
1. Treatment is not dependent on ability to pay.
2. Medicare.
3. Employer provided health care benefits and their special tax treatment.
4. Supply bottlenecks for things like doctors and nurses (we, quite literally, import nurses from places like the Philippines…or we did, not sure how the current economic situation has impacted this.).
5. Gammon’s law.
I have found 2 countries where their health care systems appear to be sustainable. Singapore (really, really tiny) and Belgium (a quite small country). Are those systems portable to the U.S.? I have my doubts. For example, Singapore relies quite a bit on forced savings/health care savings accounts and is a country with a rather different economy. And does size and culture play a role?
The bottom line is that there is no solution. Right now the best we can hope for is a holding action–reduce the cost growth rate and hope that a miracle happens. That is shit policy when you get right down to it, but that is our best option. Any other solution and that person proposing it is almost surely stuck on stupid.
I just know that finding data for things like GDP is not that easy when you get farther back in time. Spending on health care? My guess is that such data is even more difficult to track down. So, I’d take such data with some caution. And I think the original author does as well considering that they split the data into two series. It is a good sign that the data overlaps in for a significant portion of the graph, but in looking at some of the earliest data there is something funny going on (1929 – 1935).
steve,
Dude, its logged data. When you have exponential data and you take the log of that data you get a straight line. Hence a change in the slope means a change in the exponent in the underlying exponential data. Whip out Excel and graph the two functions:
f(x) = x(lagged one period)*(1.01)
g(x) = x(lagged one period)*(1.0125)
Then take logs and graph them side by side. I did it using x = 1 as a starting point. After 200 iterations the first equation works out to 7.24 and the second to 11.85. The second is about 63% larger than the first. However, after taking lags the second equation has a slope that is only 24% larger than. That is change in slope is about 1/3rd as large as the percentage difference in the actual data we are interested in. Take it out 400 iterations and the differences are even more stark the percentage difference between the two exponential equations being 168% and the slope differences still being about 24%.
In other words, a small change in the slope can have a larger impact on the actual data series we are interested in.
It may be an artifact of the data collection method but I also see a pattern that appears to be repeated every few years after 1965 in which the curve begins to level off (healthcare stabilizes as a percentage of GDP) and then takes off again to resume its path. I strongly suspect that’s a consequence of policy.
Yeah you are right about that effect, it looks small, but given the data is logged. Would be nice to have the data, fit a simple trend line and look at the residuals. The would confirm your suspicion on the presence of those surges.