An article by John Tozzi at Bloomberg Businessweek provides some useful perspective:
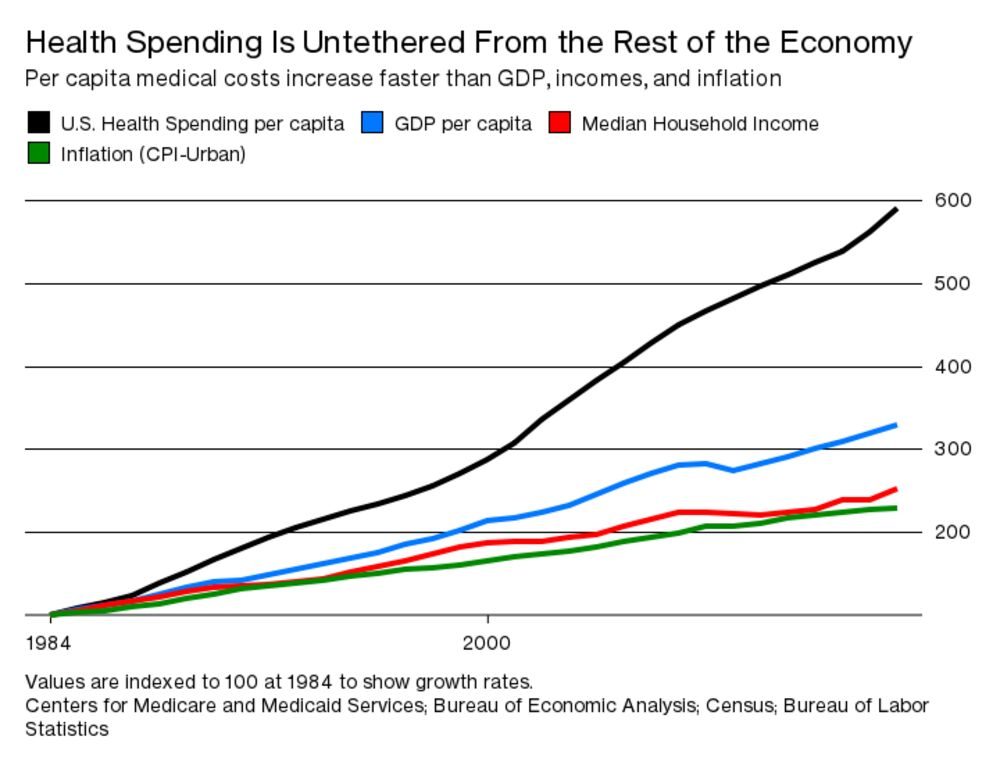
Whatever happens to Obamacare in Washington, the rest of America will be left with a problem it’s had for decades: Health-care spending is growing at an unsustainable rate. Insurance and medical costs are draining the incomes of the middle class—tens of millions of people who earn too much to qualify for government-subsidized coverage, but not so much that they don’t feel the bite of medical bills—and nothing on Congress’s agenda is likely to fix that.
That’s the point I’ve been hammering since 2010. It’s actually worse than he portrays it. Wages aren’t rising. Even when wages are flat total compensation rises because of health care unless the workers shoulder more of the expense of their own health care. If they do shoulder more of the expense of their care, that leaves less for everything else on which they might otherwise spend their money including saving. If they spend less on everything else, that leaves the non-health care economy struggling.
The situation is yet worse when it comes to investment. Health care attracts a disproportionate amount of total investment because, due to the government subsidies amounting to something between 50% and 70% of all health care spending, it’s very nearly a sure thing.
If you can figure out a way that growth in health care spending relative to everything else can continue to increase as rapidly as is reflected in the graph above, I’d like to know about it. There is no such thing as perpetual motion.






I believe higher education costs are rising more quickly than health care, but the universities get a pass from the Progressive media. The accumulated debt that recent graduates have must itself be a big drag on the economy. So, when does the Crunch happen? Does it prevent the Singularity?
We’ve had four consecutive administrations, Republican and Democratic, telling us that higher education is the key to a bright economic future. On reflection I guess it is—for bankers and educators.
Fun facts: Germany’s percentage of the population with tertiary education is just a little over half what it is here and their unemployment rate is lower than ours.
The current model is for government to print more and more dollars and continuously shovel it at the health insurance industry, hospitals and doctors.
Given the lousy return this is ultimately a subsidy to the rich and big corporations in the same way U.S. debt is a subsidy.
I fear it will end only with the guillotine.
And it’s been so successful it’s being replicated with higher education.
For most of history, much of the populace has been illiterate, and the happy admonition “Get an education, get a job!” addressed to just about anyone made complete sense. Some point in the 1990’s, however, we reached a point where the number of college educated Americans was larger than the number of jobs that actually required a college degree, and we’ve been wheel spinning since.
You’ll note that the biggest advocates of “Get an education!” tend to be older people who learned their Sacred Truths before the 1990s and who never had to rub their noses against reality. You might also note that giving this friendly advice doesn’t take anything out of my pocket, nor require any special effort on my part.
“Get down on your knees and pray!” would be equally good advice for job seekers these days, but that would sound a bit strange coming from Paul Krugman and many other education boosters.
Separating health insurance from health care is a well worn subject here and elsewhere, and deservedly so. Central issues in escalating health insurance costs appear to be government subsidy – no model of good cost stewardship – the bastardization of insurance into comprehensive maintenance.
But since insurance is just financing, what are the root causes of health care cost escalation? The statistics that the preponderance of costs are incurred in the very first and last stages of life seems a fruitful place to look. What to do about preme babies or the terminally ill in the last few months? Steve always reminds us about the disproportionate expense associated with chronic disease management (diabetes) or relatively costly surgical procedures. Is it the analog of eating on an expense account, as insurance is “free?” Will single payer really work, or will Everyman be getting their health care at Ponderosa Steak House, and the Rich at Mortons? Place your bets. What other first order issues are there?
Which one of those issues would not be addressable if insurance was really insurance, and not maintenance? And which ones unaddressable by creating real risk adjusted pools? Why shouldn’t the obese pay more in premiums? People who live in hurricane prone regions pay a lot more in homeowners insurance risk premiums you know……
Perhaps the real problem is that no one has the balls to have a frank discussion with Americans. They are getting creamed by costs, yet somehow they have convinced themselves that someone else is paying, or will pay. How’s that working out?
Getting back to the original subject matter … I think our rising medical costs show we are in a transition period (several actually). At some point, the US will have to decide whether healthcare is just some public good that should be provided to everyone, something like clean air, or whether it should continue to be a gambling enterprise for insurance companies who are often protected from failure by government subsidies. We haven’t had that debate yet, and perhaps we should.
Secondly, I’ll note the biggest costs in modern medical care seem to lie in the last year or two of the lives of elderly patients. We spend a bunch “heroically” trying to preserve the lives of the dying. This is praiseworthy in many ways, but not in other ways. It’s occasionally noted that doctors, more familiar with death and dying than most of us, when facing the ends of their own lives don’t often choose such heroic measures for themselves. Perhaps we should seek to cultivate a philosophy of “tranquil death” for the elderly and try to limit emergency measures to people young enough to get some years to come?
(Just speculating, but suppose half a dozen major Hollywood films featured some elderly protagonists dying calmly and serenely, expressing “My job is done” sentiments. Would this shape attitudes in the general public?)
Thirdly, I’ll note that medicine is a branch of biology and we’ve hardly begun to dig into that science. A lot of our medical costs come from diseases which we cannot cure, but where symptoms can be alleviated. COPD, for example (the one I know best). Other costs come from diseases we can’t really treat, or even diagnose, because they’re just too damned infrequent to deal with — think of Legionnaire’s Disease in the 1950’s, or aids before 1980. We’re going to get better at treating obscure diseases, we’re going to get better at treating chronic diseases. I think the path ahead is a difficult one, over rough terraine, with a lot of detours and false ends, but a century or so from now some parts of medicine are probably going to be quite different from today. Yeah, replacing an 80 year old’s busted hip is probably still going to be a job, but maybe obstetricians can persuade would-be parents to screen out potential fetuses with hemophilia and Williams Syndrome and Downs Syndrome and others. Maybe treating liver cirrhosis or Crohn’s disease can become as complicated as giving vitamin C to people with scurvy. There is much to took forward to!
There’s yet another possibility, of course, by no means such a happy one, where we learn that all humans are idiosyncratic to a degree, and thus that all diseases are very tied to individuals, and that treating specific diseases in each of us requires very specific medicines and forms of treatment. I THINK, from what I know of human genetics that this is not a likely future, but I have to point out it could happem.
Save me from this speculation, Steve, if you’re paying attention!
Guarnari —
Our comments seem to overlap. Apologies — I was mumbling to myself and punching away desultorily at the keyboard while you were posting.
Other hand, it’s comforting to see great minds pursuing the same course.
There are no legislative solutions here, only haggling over how much Government money and where it will go. We will all need to sort out on our own how much family resources go to extend life or nourish the next generation.
I suspect that the end of life issues are more driven by family members, and the quality-of-life issues are more driven by the individual.
If I am going to live another 5 years, I want to be able to function as independently as possible, but at some point, I will be (or am) ready to let go. What happens if I am ready to let go but family members are not?
As to general health care/insurance, one way to quickly change the debate would be to eliminate all tax-free health care/insurance spending. I suggest that many of the people who whine about “free stuff” have excluded themselves from the elimination of “free stuff”.
What happens if I am ready to let go but family members are not?
Living Will.
We don’t do too well with public goods. The highway system is a decrepit mess. We have bridges to nowhere and useless buildings, all for self aggrandizement or a politician’s construction company buddies. We are bankrupting the place with vote producing education and public pensions.
I’ve been universally shot down at Tasty’s suggestion that freebies not be Freebies. I’d note that my health insurance is considered a “partner draw,” and is taxable income.
I wrote that comment to intentionally have dead ends, because that’s where we end up. Someone usually ends up advocating the government, but it’s usually the same people who rail against the Pentagon. Go figure.
@Drew
Your free-stuff is a debt backed currency. If it were not for LBJ and Nixon obliterating any monetary discipline, you would more than likely still be working in a steel mill.
As to the tax free health insurance, you are an outlier.
@gray shambler
A Living Will only affects you when you are unresponsive. I suspect that the idea of Grandma living forever is driven by family members, and if she is going to live that long, a hip replacement or organ transplant are logical choices.